The official version of this document can be found via the PDF button.
The below content has been automatically generated from the original PDF and some formatting may have been lost, therefore it should not be relied upon to extract citations or propose amendments.
1240/5(6425)
WRITTEN QUESTION TO THE MINISTER FOR HEALTH AND SOCIAL SERVICES BY DEPUTY P.V.F. LE CLAIRE OF ST. HELIER
ANSWER TO BE TABLED ON TUESDAY 5th JULY 2011
Question
Could the Minister for Health and Social Services give the most current figures for each type of cancer in Jersey and also indicate the age brackets for each type of cancer? Does the Department maintain data on how the figures and age brackets compare with the UK and the neighbouring region of Normandy?
Answer
Cancer Information
Locally statistics on cancer incidence (the annual number of new cancers diagnosed) and cancer mortality (annual deaths) are maintained by the Health Intelligence Unit within HSSD. This data is collated and analysed to look at trends and compare with other areas where possible. Because of the small numbers for some cancers annual rates do vary from year to year so it can be difficult to get an accurate picture of what is happening.
Cancer Incidence
The statistics for incidence of new cancers in Jersey are contained within the regular reports produced for us by the UK South West Cancer Intelligence Service. The latest Channel Islands Cancer Registration Report 2010 covers the three year period 2005 - 2007 and is available on from:
http://www.gov.je/Government/Pages/StatesReports.aspx?ReportID=538give link
This report showed that the main cancers diagnosed in Jersey in 2005-07 were non malignant skin cancer, lung cancer, breast cancer, prostate cancer, colorectal cancer, malignant melanoma and blood cancers (see p7 of report).
Table 1 summarises the information from this report for the 5 main malignant cancer types diagnosed in Jersey.
Table 1: Summary of the main malignant cancer types diagnosed in Jersey
Cancer site | Annual average no. of cancers diagnosed |
|
| By age group | ||
0-19 | 20-64 | 65+ | ||||
Breast (F) | 65 | 113.5 | low | 0 | 46% | 54% |
Prostate (M) | 74 | 146.2 | high | 0 | 28% | 72% |
Lung | 61 | 55.7 | high | 0 | 29% | 71% |
Colorectal | 51 | 43.4 | ns | 0 | 37% | 63% |
Skin Malig.Melanoma | 35 | 34.3 | high | 3% | 58% | 39% |

Data shows that 1% of all new cancers occurred in the under 20's, 40% in those aged 20-64 years and 59% in the over 65's. This is a similar pattern to Guernsey & the South West.
Analysis carried out by the South West Public Health Observatory over the years has shown that Jersey has rates of cancer roughly comparable with the mainland and Guernsey for colorectal cancer, gynaecological cancer, leukaemia and upper gastro-intestinal cancer and, more recently, slightly lower for breast cancer incidence.
Incidence rates were significantly higher in Jersey than the South West for lung cancer, head & neck cancer, malignant skin melanoma, stomach cancer, prostate cancer and testicular cancer in 2005-07 (see p13 of the report for full details). However, the numbers for some of these cancers are low so the data must be treated with some caution.
Higher incidence rates are not always a bad thing. If an area has better systems in place to detect a certain cancer and/or specialists skilled in diagnosing that cancer then more people will be picked up with it. High incidence rates can indicate better detection of a cancer. Early detection of cancer can led to better outcomes & cure.
The Health Intelligence Unit is working on finding reliable European data (including French regions) for further comparison. Such data is not always suitable for comparative purposes due to differences in the way it is collected, coded or analysed. For example French cancer incidence data is patchy across the various regions and does not cover all cases (unlike the UK & Jersey where almost 100% of cases are picked up by a robust cancer registration process).
Cancer Mortality
Mortality data is collated and analysed annually by the HSSD's Health Intelligence Unit.
Jersey data shows that lung, upper gastrointestinal (oesophagus, stomach & pancreas) and colorectal cancers contribute to almost half of all cancer deaths in Jersey. This reflects world wide and European trends where lung cancer the single main cause of all cancer deaths.
Cancer of digestive organs (including upper gastrointestinal and colorectal cancers) accounts for a quarter of all Jersey deaths due to cancer. The second most common cause of cancer death is cancers of respiratory organs (mostly lung cancer) at 24%, followed by female breast cancers at 9% and male genital cancer (mostly prostate) at 7% (See Figure 1).
Figure 1: Jersey cancer deaths by site (2005-09)
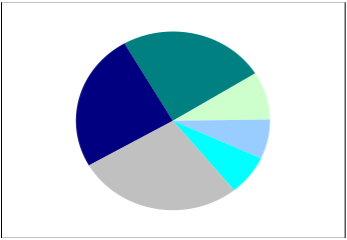 Respiratory 24%
Respiratory 24%
Digestive Breast 25% 9%
Male genital 7%
Lymphoid, haematopoi
etic tissue All other 7%
sites
28%
In terms of the age groups affected HSSD's Health Intelligence Unit maintains detailed spreadsheets for the main cancer sites by age group with data going back to 1996. This allows in depth analysis of individual cancers as required. From this we can show that nearly 60% of all cancer deaths in Jersey occur in those aged 70 or over and we have very few cancer deaths under aged 40 (Table 2).
Table 2: Jersey cancer deaths by age (2005-09)
Age group | Total (2005 – 2009) |
|
|
under 20 | 3 | 1 | 0.3% |
21-39 | 12 | 2 | 1.2% |
40-59 | 185 | 37 | 17.9% |
60-69 | 230 | 46 | 22.2% |
70-79 | 296 | 59 | 28.6% |
80+ | 309 | 62 | 29.8% |
Figure 2: Cancer deaths by age group 2005 – 2009
 Average number of annual cancer deaths by age group (2005-09)
Average number of annual cancer deaths by age group (2005-09)
100 90 80 70 60 50 40 30 20 10
| ||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0
1-4 5-9 9 -24 29 34 4 -49 54 59 9 -74 75+ year 10-14 15-1 20 25- 30- 35-39 40-4 45 50- 55- 60-64 65-6 70
<1
Using Incidence & Mortality data
Ideally cancer incidence and cancer mortality should be looked at together.
A high incidence rate and an equally high mortality rate would indicate that that cancer was a particular problem, for example lung cancer.
But a high incidence rate can also be due to better diagnosis and detection of a cancer, and, if linked with lower mortality rates, indicate better treatment of those cancers, for example breast cancer.