The official version of this document can be found via the PDF button.
The below content has been automatically generated from the original PDF and some formatting may have been lost, therefore it should not be relied upon to extract citations or propose amendments.
Peter Crill House Gloucester Street St Helier
Jersey, JE1 3QS
Deputy Raluca Kovacs
Lead Member States Annual Report and Accounts 2023 Review States of Jersey
BY EMAIL 17 June 2024
Dear Deputy ,
States Annual Report and Accounts 2023 - Response
Thank you for your letter dated 3rd June 2024, regarding Health and Community Services' contribution to the 2023 Annual Report and Accounts. Please find my response to your questions below. If you require any further information, please do not hesitate to contact me.
C&AG Recommendations
- The PAC notes that 10 recommendations in relation to the Deployment of Staff Resources in HCS had their target dates revised to 2024 from 2023. Furthermore, one recommendation related to the Learning from Previous Hospital Projects – a follow up review, has had the target date revised to 2024 from 2023. What were the reasons for the revision of the target dates for these recommendations into 2024?
The recommendations made by the Comptroller and Auditor General in their Deployment of Staff Resources' review, were received by HCS at the beginning of 2023 - a period of significant change in the Department, due to the response to the Review of Clinical Governance Report [1]and the start of the turnaround team and programme.[2]
Overall, limited capacity and/or available specialist skills were contributing to the need to revise the target date. In addition, the time required for staff engagement was underestimated. As a consequence, the below activities and recommendations have had their target delivery date amended:
• develop a strategic workforce plan (recommendations 2,3 and 4)
• review and, where appropriate, negotiate the terms and conditions of HCS staff (recommendation 5)
• develop of a clinical supervision policy (recommendation 15 and 16).
• clinical practice of locum doctors (recommendation 17)
• review of compensation for on-call (recommendation 18)
However, since the publication of the Annual Report, considerable progress was made against the following recommendations which have now been completed:
Deployment of staff resources:
Recommendation 7: the Private Patients Strategy [3]has been completed and published.
Recommendation 9: the HCS Annual Plan [4]includes an organisational development and culture plan (pages 139 to 142 of the Board papers).
Learning from Previous Hospital Projects – a follow up review' Recommendation 4: the functional brief has been updated. Patient Waiting Times
- Has the introduction of the Electronic Patient Record system reduced patient waiting times for:
Waiting times for outpatient and inpatient appointments are now being monitored through the electronic patient record system (EPR). In May 2023, the TrakCare software was replaced with the Maxims software. The new Maxims EPR uses a patient-focused approach which enables better clinical oversight of patients' pathways and operational management of activities. The waiting list numbers have been affected due to this change. I have therefore included details on the difference between the two systems in the answer below.
- Outpatient appointments?
The Maxims Electronic Patient Record (EPR) is a referral-based patient record system that allows patients to be tracked through an entire pathway from referral to treatment and post treatment care before being discharged from the consultant's care. Our previous Patient Administration System (PAS) (TrakCare) was an episode based system, which means that each part of the pathway (outpatient activity, diagnostics, pre-assessment activity, inpatient activity, therapy input) was recorded separately – and sometimes a patient had multiple episodes for the same care pathway.
New/First Outpatient Patient Tracking List (PTL)
As the new system is referral based, all activity must have a referral created in order to be able to book an appointment. This was not required in TrakCare where this referral step was often bypassed, and an episode created to record the activity against – in this case we were unable to report a patient as being on the waiting list and unable to calculate the time from the referral being received to the patient being seen. The rigour of creating the referral in Maxims has led to an increase in the waiting list numbers as part of the Maxims EPR implementation – however, the numbers much better reflect the actual number of patients waiting to be seen in secondary care.
There were a number of issues identified in the few weeks immediately after Go Live that further inflated the numbers briefly – but each of these has been systematically addressed with a full issues log documented in relation to the issue, including root cause analysis and any fixes applied.
First Outpatient Attendance Waiting list counts and waiting times (% waiting greater than 90 days) as published in the 2023 Month 12 Quality & Performance Report:


This shows that there has been an increase in the volume of patients waiting for a first outpatient appointment at the acute hospital, but a decrease in the number waiting for an appointment in our Community specialties (mainly Dental and Physiotherapy) – the decrease is driven by the impact of the waiting list recovery plan.
- Operations?
The Elective Waiting List has also grown over 2023 but not by as much as the outpatient waiting list. Patients are only added to the elective list once they have been seen in outpatients.
Activity was reduced immediately after the EPR implementation to enable an embedding period, the impact of this is illustrated in the waiting list growth in June with a decrease in August as activity returned to normal levels. The growth in the later months of the year reflects increased outpatient activity which has converted to elective waiting list requests.

![]()
- How much have waiting lists deteriorated' in 2023 & in which areas?
From 2024 we started reporting median waits at month end. Data are published at specialty level on gov.je within 5-10 working days of the month end.
Note: The median wait shows the typical length of time a patient has been waiting – it indicates that half of the patients are waiting less than the number of weeks and half the patients are waiting longer.
The median waiting time in weeks for First Outpatient Appointment (all specialties, acute and community), month end snapshot:
Jan-23 | Feb-23 | Mar-23 | Apr-23 | May-23 | Jun-23 | Jul-23 | Aug-23 | Sep-23 | Oct-23 | Nov-23 | Dec-23 |
10 | 10 | 8 | 9 | 10 | 10 | 11 | 11 | 12 | 12 | 11 | 13 |
The median waiting time in weeks for First Outpatient Appointment varies by specialty – selected specialties where there has been an increase or decrease in median wait over 2023 are shown below:
Specialty | Jan | Feb | Mar | Apr | May | Jun | Jul | Aug | Sep | Oct | Nov | Dec |
Clinical Genetics | 86 | 90 | 91 | 76 | 72 | 75 | 78 | 80 | 78 | 78 | 54 | 57 |
Community Health Services Dental | 55 | 55 | 51 | 52 | 53 | 53 | 56 | 53 | 43 | 40 | 32 | 30 |
Dermatology | 10 | 7 | 8 | 9 | 10 | 11 | 13 | 13 | 15 | 18 | 20 | 23 |
ENT | 7 | 7 | 7 | 9 | 10 | 10 | 12 | 12 | 15 | 16 | 16 | 17 |
Gastroenterology | 6 | 6 | 5 | 6 | 7 | 11 | 9 | 9 | 11 | 16 | 17 | 16 |
Neurology | 4 | 4 | 3 | 5 | 4 | 5 | 8 | 8 | 9 | 12 | 9 | 11 |
Ophthalmology | 33 | 35 | 31 | 32 | 31 | 24 | 25 | 25 | 26 | 29 | 25 | 24 |
The median waiting time in weeks for Elective Admission (all specialties) month end snapshot:
2023 | |||||||||||
Jan | Feb | Mar | Apr | May | Jun | Jul | Aug | Sep | Oct | Nov | Dec |
14 | 15 | 17 | 15 | 16 | 16 | 15 | 17 | 16 | 17 | 16 | 16 |
The median waiting time in weeks for Elective Admission varies by specialty – selected specialties where there has been an increase or decrease in median wait over 2023 are shown below :
Specialty | Jan | Feb | Mar | Apr | May | Jun | Jul | Aug | Sep | Oct | Nov | Dec |
Community Health Services Dental | 1 | 4 | 7 | 11 | 13 | 4 | 3 | 1 | 3 | 3 | 3 | 4 |
Dermatology | 8 | 5 | 6 | 7 | 9 | 9 | 7 | 11 | 13 | 16 | 3 | 7 |
General Surgery | 16 | 17 | 19 | 20 | 22 | 22 | 23 | 23 | 23 | 23 | 22 | 22 |
Ophthalmology | 16 | 16 | 17 | 16 | 14 | 15 | 14 | 15 | 14 | 13 | 11 | 11 |
Trauma & Orthopaedics | 20 | 19 | 21 | 23 | 21 | 23 | 24 | 25 | 22 | 21 | 21 | 21 |
Urology | 10 | 6 | 7 | 6 | 8 | 9 | 8 | 8 | 8 | 6 | 5 | 7 |
- How long are patients waiting for their first acute patient appointment?
See tables above. For latest data, see also Hospital waiting lists' on gov.je https://www.gov.je/Health/WaitingLists/Pages/HospitalWaitingLists.aspx
- Has the development of patient level information and costing system (PLICS) identified whether HCS has enough capacity to meet referral demands for individual purposes?
PLICS does not provide the answer to this question, instead HCS uses capacity and demand modelling to understand overall capacity issues. Based on the modelling, and as seen in the above median waiting time tables, capacity is different across all specialties.
On an individual basis, every patient is clinically assessed and placed on the waiting list according to their medical assessment. Urgent cases are always prioritised. Clinical assessment of patients on the waiting lists is regularly undertaken.
Overall capacity issues, particularly in outpatients, are being addressed through the outpatient improvement programme which focuses on implementation of more efficient ways of working. In addition, capacity issues have been addressed through the waiting list initiative where some activity is transferred to the UK (for example, Ophthalmology).
Operating Theatres
- How many operating theatres are there currently? There are seven theatres in total, consisting of:
- three elective operating theatres in Main Theatres, with
- one general elective theatre,
- one dedicated obstetric theatre, and
- one dedicated emergency theatre,
- two elective operating theatres in the Day Surgery Unit (DSU),
- one Minor Operations theatre, and
- one operating theatre that is not in use, due to recruitment and staffing issues.
- What is the active period in a normal week?
The theatre opening times are:
- Elective Theatres (General & Obstetrics):
o Monday to Friday: 08:30 – 17:00
o Currently, we can operate over-runs' on Tuesdays and Wednesdays for public and private waiting lists.
- Elective Theatre (Emergency):
o Open 24 / 7
- Day Surgery Unit:
o Monday to Friday: 08:30 – 17:00
o Saturday: 08:30 – 13:30
- Minor Ops:
o Monday to Friday: 08:30 – 17:00
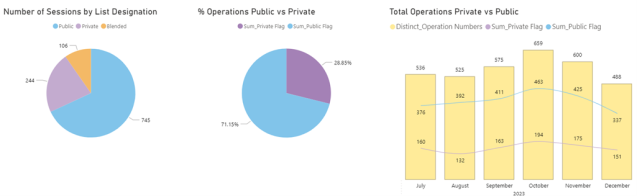
- What is the percentage of use by:
- public
- private patients
Theatre use can be shown in two different ways. Firstly, they can be considered at session level - in the first pie chart, sessions are shown by list type (or designation), i.e. they are either public, private or both (blended).
Secondly, as shown in the second pie chart and the bar chart below, the split of public and private procedures can be shown as they have actually happened. Each procedure will either be public or private. This shows that the majority of procedures have been undertaken are publicly funded.
Data are shown for July – December 2023.
- Theatre utilisation has been identified as 73.6% in quarter 1 dropping to 66% in Q4 what has, or is being done to achieve a target above the 85% threshold?
A theatre efficiency programme is in place and has seen a steady increase in utilisation month-on- month since December 2023. The Q1 position 2023 was taken from the old PAS system (TrakCare), which did not accurately reflect the position. We are now assured that data collection is more robust, and we are seeing the correct position. The utilisation report also includes private theatre time. Since the introduction of blending private and public lists (implemented June 24), it is anticipated utilisation will increase.
Outpatient and elective admissions
- The diagnostic patient tracking list showing patients waiting more than 90 days for a diagnostic procedure has a target of 25%, in Q1 it was 49.6% in Q2 = 70.8% and Q4 = 66.3%. What has or is being done to improve this situation?
Diagnostic capacity versus the demand remains challenging. Waiting list initiative schemes across endoscopy and Magnetic Resonance Imaging (MRI) have been undertaken at the end of 2023 and into 2024. These two schemes resulted in significant reduction in waiting list size. A new gastroenterologist has been appointed with a start of July which will improve capacity in endoscopy, and an approved business case for increased MRI capacity, with a commencement of recruitment started, will ultimately improve MRI access times.
- Challenges have been identified across speculation with patients waiting more than 90 days for elective admissions, although the target is less than 25%, the Q1 figure was 56.1% and the Q4 figure was 56.7%. What is being done to produce outcomes in time with the 25% target?
Extensive Waiting List Initiatives (WLI) initiatives have been implemented across specialties in recent months, with work continuing to reduce the long waits. In addition, we are working on improving theatre efficiency and utilisation which will have a positive impact on reducing waiting times.
- Outpatient appointments show that the percentage of patients waiting more than 90 days has a target of 25% of the list. The Q4 figure was 48.2%. What is being done to improve this?
In addition to the Waiting List Initiatives, an extensive programme is in place to support outpatient waiting times improvement and includes:
• clinic template reviews,
• capacity and demand management,
• improvement of outpatient estate utilisation,
• recruiting substantively into consultant posts to improve continuation of services,
• development of a centralised referral hub,
• standardised clinical administration processes,
• Outpatient Department (OPD) Nursing staff responsibility review,
• phlebotomy processes to improve diagnostic, and
• reduction of non-attendance of appointments (DNA rate).
- Outpatients not attending outpatient appointments was recorded at 10.7% at the end of 2023, with the introduction of the new Electronic Patient System, whereby patients need to "opt in" to receive texts, reminders etc. What is being done if anything to improve this situation?
The Did Not Attend (DNA) rate remains static, this Key Performance Indicator (KPI) is included in the improvement work being done in the outpatient improvement programme. Patients who provide their mobile number and give permission for us to send them a text reminder remains in place. The new patient access policy provides a more robust process around patients that did not attend their appointment, and ensures patients are aware of the impact of missed appointments.
- The target for non-attendance at booked appointments for under 18's was 8.7% in 2023, although the year end showed the average over the year was 15%. What is being done to achieve better attendance?
Text reminders for outpatient appointments have been introduced (to parents) and phone call reminders to parents for inpatient appointments have started. In addition, we are considering the offer of more convenient appointments such as after school and during term holidays.
Please note that whilst percentages for non-attendance may have been high, overall numbers are very low across the majority of specialties. As total appointment numbers are low for children across most specialities, non-attendance of a few will show as a high percentage.
To put this into context, in Trauma & Orthopaedics attendance numbers are usually the highest among all specialties. In May 2024, the was not brought' rate for children under 18 was under 7%.
Regardless of numbers, the process for safeguarding children, should concern be raised by the clinical teams, remains in place.
- What measures are being taken, if any, to achieve better outcomes per patients with reduced waiting times for appointments, operations and procedures?
Every patient is medically assessed and prioritised based on clinical need to ensure best health outcomes. In order to reduce waiting times across outpatients, diagnostics and elective appointments, a number of actions are being undertaken, please see above answers for the details.
Additional questions
- Can you please confirm whether you are providing quarterly reports to Ministers in relation to performance/budgets, and in what format do these briefings take place?
The department currently has weekly briefings with the Minister to brief him on operational, performance and finance matters. Additional briefings are being arranged if required. HCS currently submits performance and finance reports to the HCS Advisory Board,[5] which are shared with the Minister and Assistant Ministers for Health and Social Services. The Minister regularly meets with the non-executive Directors of the Board to be briefed.
- Are there any areas where performance has been affected since the re-prioritisation of the Government Plan?
Monies were provided in the 2024 Government Plan for the Strategic Health Policy Team (Cabinet Office) to undertake a programme of work. That programme of work has been subject to some changes, most notably the decision not to progress with the development of a standalone women's health strategy. This decision was taken at the end of 2023 by the previous MHSS but not communicated until 2024 once the decision had been discussed with the Women's Health Political Advisory Group. This decision does not directly affect the performance of HCS in the short to medium term but may have had longer term impact if it is assumed that strategy was to include matter related to HCS delivered women's health services.
- Which departments gave briefings to their respective Minister in relation to their performance across 2023? Can the PAC also be provided with links to these briefings in confidence for its own awareness/information?
HCS officers provided regularly briefings to the MHSS on the HCS performance using the Quality Performance Report (QPR), the reports can be found here: https://www.gov.je/health/waitinglists/pages/quarterlyperformancereport.aspx
Since October 2023, the briefings included all papers that were discussed at the HCS Advisory report including the QPR: https://www.gov.je/government/departments/healthcommunityservices/pages/healthcommunityser vicesdepartmentboardmeetingpublic.aspx
The MHSS was also briefed on the performance against the Ministerial Plan. An end of year report on the 2023 Ministerial Priorities was provided to the Health and Social Services scrutiny Panel on 11th January 2024, it can be found here:
Delivery Plan 2023 reporting - Min for Health and Social Services.xlsm
Yours sincerely

Chris Bown
Chief Officer, HCS
D +44 (0)1534 442272 E c.bown@gov.je
[1] Review of Health and Community Services (HCS) Clinical Governance Arrangements within Secondary Care
[4] HCS Advisory Board - Papers - Part A - May 2024.pdf (gov.je) pages 139 to 142 of the HCS Board pack