The official version of this document can be found via the PDF button.
The below content has been automatically generated from the original PDF and some formatting may have been lost, therefore it should not be relied upon to extract citations or propose amendments.
19-21 Broad Street | St Helier Jersey | JE2 4WE
Deputy Rob Ward
Chair, Safer Travel Guidelines Review Panel
BY EMAIL
28 July 2021 Dear Chair,
Thank you for your letter of 1July and apologies for the delay in my reply. You raised a number of queries and requested information on a number of points, each of which is addressed below.
• What proportion of vaccinated Islanders will be considered sufficient to establish community immunity and when do you anticipate that this will happen?
The calculation of community immunity (or population' or herd' immunity) has been made more complex by the increased transmissibility of the Delta variant. New and emerging evidence of the infection rate of the virus (without the effect of immunity) suggests that the delta variant has a reproduction number (Ro) of around 7 (see the latest SPI-M-O estimates) whereas the original wildtype variant is estimated to have an Ro of 2.5. Calculations also need to include the latest vaccine efficacy estimates. The reduction in the reproduction number afforded by NPIs is estimated based on the latest SPI-M-O reports, with the Imperial College Modelling Group estimating that test, trace and isolate will reduce transmission by approximately a third. Given recent changes in the approach of contact tracing, it is difficult to estimate the future reduction in transmission afforded by the local test, trace and isolate system. Other NPIs, such as reduction in household gatherings, social distancing and the wearing of masks also have an effect on reducing transmission. Therefore, it is hard to estimate the exact infection rate of the virus (without the effect of immunity) in order to calculate a level of community immunity.
A range of scenarios for herd immunity were presented to STAC on the 21 June 2021, based on an estimate that vaccination provides full immunity in 95% of those vaccinated.
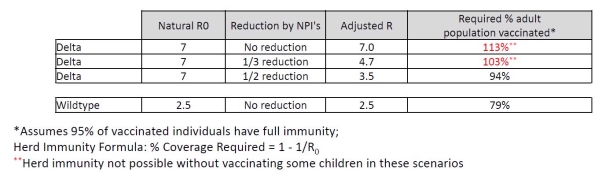
63% of the adult population have been fully vaccinated in Jersey (as of 4 July 2021), so it is clear that community immunity has not yet been realised.
According to Public Health England, vaccine efficacy against symptomatic infection is considered to be 80%, against hospitalisation 96% and against death 98%.
Currently < 18yr olds cannot be vaccinated (unless very vulnerable) i.e. only some 80% of our population is eligible for vaccination. But disease has been shown to be generally much milder in young people.
• What impact will full vaccination offer in the reconnection strategy and longer-term response to COVID-19?
Full vaccination coverage will facilitate reconnection by significantly reducing severe disease and hospitalisation. It will not ablate infection or all severe disease.
The variations to isolation requirements under the Safer Travel Policy are based on an assessment of risk based on passenger profile, including vaccination status and travel history with a subsequent risk assessed requirement for testing and isolation.
• What action is being taken to vaccinate Islanders who are under the age of 18?
Government of Jersey policy is to follow the Joint Committee on Vaccination and Immunisations (JCVI) and UK authorities on COVID19 vaccinations. The JCVI is advising that those who are under 18 do not receive any of the vaccines unless they are in priority 4 (clinically extremely vulnerable) or priority 6 (those with underlying conditions who are more susceptible to COVID-19). In addition, young people aged 16-18 years, who are employed in, studying or in training for health and social care work have also been offered vaccination alongside their colleagues. The numbers in this group are very small (<1%).
• Is the Government of Jersey investigating a programme of vaccination for 12- to 18- year-olds?
The current policy on under 18-year olds is being reviewed by the JCVI currently and we are awaiting imminent advice from the committee, which has been reviewing the evidence and risk/benefits of vaccinating under 18 years old. The current advice is to only vaccinate 16-18 years who have High Risk conditions. Once the updated advice is published by the JCVI, the Government of Jersey and the vaccination programme will review the guidance and determine how best to proceed.
• Is there a conscious move to allow COVID-19 to spread amongst under 18's due to lack of serious illness in that group and will how policies relating to those under 18 be changing during the summer?
A balance of harms approach has been taken towards the COVID-19 pandemic in Jersey. The primary focus has been on minimising death and hospitalisation due to serious illness. This has been balanced with the need to protect the wellbeing of all islanders when stricter mitigation measures were in place, such as lockdown. Through the successful roll-out of the vaccination programme providing a degree of population immunity, we are starting to see a reduction in the rate of hospitalisations even with the current increase in infections.
Public health measures remain recommended to minimise the spread of infection across all age groups, even those vaccinated. Good hand hygiene, face coverings in crowded spaces, maintaining physical distancing and allowing fresh air to circulate will help to minimise the spread of infection. Polices remain under constant review given the uncertainty of the global pandemic and the rapidly changing situation. The emergence of new variants of COVID-19 requires an ongoing risk assessment-based approach.
Some people will not be eligible for vaccination. Such individuals will become infected at some point – if they are, then it is better to be infected during the summer when there are fewer concomitant respiratory viruses.
• What level of understanding is there on the long-term impact of COVID-19 on young people, as an illness and more widely?
Most children are asymptomatic or will exhibit mild symptoms from COVID-19 infection. The long- term health implications for some children who have been infected with COVID-19 remains uncertain. As COVID-19 is a new disease the full extent of the long-term implications will not be known for some time. This therefore remains an area of uncertainty and emerging evidence. There is preliminary evidence that long COVID can affect children. The Office for National Statistics estimates that approximately 8% of those aged 2 – 16 years will go on to experience long COVID (i.e. 1 in 12). A small number of children have also been identified who develop a significant systemic inflammatory response, paediatric inflammatory multisystem syndrome temporally associated with COVID-19 (PIMS-TS or PIMS). The impact on the mental health of children and young people through measures such as lockdown and prolonged periods of isolation have been well described and require an informed, proportionate policy response.
• What monitoring is conducted to make sure that tests undertaken are effective enough to gather a sufficient swabbing sample. It is the Panels' understanding that a number of positives have been identified after 5, 8 or 10 days, potentially due to lack of detection at day 0 tests;
The sensitivity of testing depends on the situation and type of test employed. PCR testing is the most sensitive. Antigen testing is about 90% as sensitive. Testing a symptomatic individual if undertaken correctly will pick up the vast majority of COVID positives (if symptoms are due to COVID).
For contacts of a positive case see below.
Not everyone will test positive on day 0 after exposure to the virus as it can take a number of days for the virus to produce enough viral particles to be detected by tests. As shown in the diagram below from the British Medical Journal:
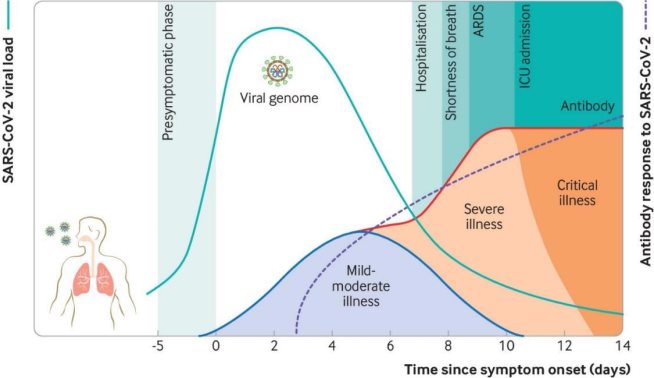
The below infection curve indicates the proportion of cases that will be picked up after exposure to the virus. It is anticipated that around 60% of cases are identified by day 5, around 85% by Day 8 and around 95% by day 10. Therefore, it should be expected that a proportion of individuals go on to test positive after a day 0 negative test.
![]() 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0%
100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0%
|
|
|
|
|
|
|
|
|
|
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
![]() % of cases Days since exposure
% of cases Days since exposure
• The Panel appreciates that some changes may need to be made at short notice. However, in line with the States approval of Part C of P.34 would be grateful for an update on the next scheduled and anticipated announcements in relation to changes to the Safer Travel Policy.
Every effort is made to ensure relevant briefings are held in advance of any public announcements or significant changes to policy, allowing for the highly dynamic situation and the need on occasion to act without delay.
I hope this information is useful to the work of the Panel. Yours sincerely,
![]()
Senator John Le Fondré Chief Minister