The official version of this document can be found via the PDF button.
The below content has been automatically generated from the original PDF and some formatting may have been lost, therefore it should not be relied upon to extract citations or propose amendments.
Report for Scrutiny of the Baby Steps Programme
Sept 2019.
Background.
The Baby Steps programme was launched initially in September 2013 by the NSPCC, as a targeted service, aimed at parents who are considered more vulnerable or challenging to engage in traditional antenatal education. It ran successfully over a four year period until October 2017 and engaged 523 adults within 34 group provisions during that time.
In April 2017 the then States of Jersey announced more than £400,000 would be released to fund the Baby Steps programme to be offered universally (to all expectant parents) delivered through Family Nursing & Home Care. From October 2017 the programme was delivered as a universal service meaning the criteria for inclusion on the targeted programme was removed (see appendix 1) and all parents were eligible to attend. Those more vulnerable clients were to remain within the universal provision. This was done as part of the transition to
the service being commissioned by the States of Jersey and delivered by Family Nursing and Homecare (FNHC).
A transition period commenced and NSPCC scaled up the offer and this involved a partnership approach between NSPCC and FNHC from October
2017 to December 2018. Full scale up and roll out of the universal service by FNHC began in January 2019.
The rational for choosing the Baby Steps programme was driven by the fact that it was identified as one of a very few evidence-based perinatal parent education programmes with recognised child and family outcomes. It was also used as part of the1001 Critical Days Agenda by key stakeholders, at all levels. There was also acknowledgment that it had been well established on Jersey over a four year period and so was potentially more acceptable to islanders and was adaptable to expansion. Reassurance was provided, as the programme had already been made universal in Blackpool and this area became a link for peer learning and development in the initial set up.
Governance and quality.
Ongoing support is offered through FNHC who holds the NSPCC license for delivery of the programme and evidencing its requirements through audit with NSPCC; whilst also being scrutinised within the current commissioning process. Quarterly strategic multiagency steering groups operate to monitor the progress of the implementation. Staff are supported through a robust supervision process provided by Baby Steps and safeguarding.
Staff undergo five days of comprehensive training in order to deliver the content of the programme, to enable them to work effectively with families and collect meaningful data and feedback. The application of various tools to evidence outcomes is necessary.
An additional strength to the implementation of the programme is that it is embedded within the existing universal service provision, delivered by health visitors and midwives and co facilitated by practitioners with a relevant health, social care education background. This approach supports the achievement of positive outcomes, as this provides seamless care for parents at the very earliest opportunity which is ongoing and supported experienced health visitors delivering the Healthy Child Programme (DOH 2009).
Baby Steps is currently the only Government provision for perinatal parent education.
The offer
Pregnancy and the first few months of a baby's life are an extremely important time for families. The early transition to parenthood is often called the perinatal period. For babies it's a time of incredible growth, which can shape their later development and influence wellbeing. For parents, it's a time of significant adjustment, as well as potential stress. Fortunately, the antenatal period is a time when parents report being open to support, and as expectant mothers receive a lot of professional contact, it is considered an opportune time to implement prevention programmes.
The baby Steps programme provides a universal perinatal education programme open to any pregnant mother resident in Jersey. The programme l covers traditional antenatal education issues including birth, breastfeeding, and practical baby care, the Baby Steps programme also aims to strengthen known protective factors in the perinatal period which include:
• Strengthening parent-infant relationships
• Strengthening couple relationships
• Building strong support networks
• Improving feelings of self-confidence as well as levels of low mood and worry
• Helping parents understand baby's development
Gaining parental consent is a standard for delivery and includes consent for information sharing e.g. from referring midwife to receiving Baby Steps practitioner and consent to participate in the programme.
The Baby Steps trained practitioners lead on each of the nine sessions that make up the Baby Steps Programme which focus on the five key themes that promote known protective factors during the perinatal period. Six sessions are antenatal and 3 sessions post birth. Groups are no larger than ten mothers/partners.
These include
• Parent Infant Relationship: From the start of the programme parents are encouraged to think about what their baby may be like as an individual and how he/she might be influenced by what is happening in their environment. After babies are born, they need caregivers to recognise and respond appropriately to their feelings and needs. Baby Steps Practitioners will work with parents to take a reflective stance and be curious about their baby's feelings. Baby Steps Practitioners will use film of parents and their babies to interpret their babies' cues and reflect on interactions.
• Couple Relationship: The transition to parenthood can be difficult and disruptive at times. Family discord can have a negative effect on child development. The Baby Steps Practitioner will encourage both partners to attend together and prepare for the new experiences that may put pressure on their relationship; explore the features of healthy relationships, and spend time actively listening to their partner, friend or family member. The Baby Steps Practitioner will reach out to involve dads and partners.
• Building Social Support: The Baby Steps Practitioner will ensure that each group session has time to enable mothers to share and listen to each other experiences in a non-judgemental and support, friendly environment.
• Emotional Wellbeing: Baby Steps Practitioner's will work with parents to develop skills and knowledge about their own emotional health by encouraging parents to talk about their feeling and emotions during each session. Practitioners will lead areas for discussion and self-help skills such as simple relaxation techniques, basic mindfulness etc.
• Understanding Babies Development: The Baby Steps Practitioner will support parents to understand and respond to different aspects of baby's development. They will be helped to understand their own expectations of their baby's development which may include factual information about different aspects of child behaviour and their development.
.
![]() The Programme details and team
The Programme details and team

The Referral pathway
Referrals will generally be completed at the 16 week booking-in' meeting which is completed by the Midwife. Other care professionals or families themselves can also contact the Baby Steps Coordinator directly and book on to the course. The expectant mother will be telephoned by Family Nursing and Home Care before the 26-week Community Midwife appointment to arrange a home visit to explain the programme in detail and consent to participate in the programme will be obtained.
An initial explanation of the programme will be offered by the Midwife and/or GP at booking and again ideally during the first and second trimester.
Mothers are encouraged to participate, but do have the choice to opt out of the programme following the initial invitation and at any stage of the programme. It is preferred that 6 of the 9 sessions are completed.
If the parent does not wish to receive the service, or commences the programme but does not complete it, Universal Health Visiting Service will be maintained as per Healthy Child Programme
Set up and delivery following transition to FNHC (Jan 2019).
Venues are east, west of the island and a venue in town is still being sought. A no cost option is being pursued as there is no identified funding for non-staff resource.
To deliver the universal programme (not from the NSPCC base), £10,000 was fund raised by FNHC charity for 2019 in order to cover costs
Client resources handed out to each parent as part of the experience
Baby demonstration equipment
Laptops and mobile phones for staff
Off island staff training with the NSPCC.
Venue resource such as visual presentations/photos/posters.
(This is not an exhaustive list).
What transition from a targeted to universal programme period told us?
A review of the transition period and the universal offer October 2017 to December 2018 was compared with the period 2015 to 2017 when the programme was targeted. Four groups were analysed including targeted mother, targeted fathers, universal mothers and universal fathers. The purpose of which was to establish:
• whether there were any significant differences in the outcomes achieved for parents receiving Baby Steps as a universal service compared to those who received it as a targeted service
Baby Steps delivered in Jersey was viewed as a useful course which could help to prepare parents for having a baby. There were mixed feelings about some aspects of the course, such as the sessions on birth, but aspects of the course which respondents rated as helpful were the group discussions and practical support on tasks such as bathing. Some respondents suggested that more advice on other practical issues such as breastfeeding and colic would have been beneficial. This adaptation has since been made.
The targeted groups appeared to have higher levels of initial needs than the universal groups, as they had higher levels of depression, anxiety and were more likely to be smokers, young parents and have had children's service involvement. Most universal parents did not appear to suffer from depression, though 42% of universal mothers had some degree of anxiety.
There were significant positive improvements in anxiety and depression scores for mothers who had attended the universally delivered Baby Steps and fathers who had attended the targeted service. There was also a Time Line 1 (data collected at session 1) to Time line 2 (data collected session 6) reduction in anxiety scores which was approaching significance for the targeted mothers. However, by the end of the programme there was very little change between targeted mothers' depression and anxiety scores. As these individuals were selected for this programme based on vulnerability' criteria, and because these mothers had higher initial levels of depression and anxiety than the other groups, perhaps Baby Steps alone is not sufficient to significantly reduce these difficulties and additional support may be needed. Additionally, a small proportion of individual's scores indicated they were more anxious or depressed after the programme. Research indicates that both pregnancy and the post- partum period is a particularly vulnerable time to develop mood and anxiety disorders, therefore this may explain why some women's scores worsened.
There were no significant differences between the reduction of anxiety and depression scores between families who attended Baby Steps as a universal service compared to those who attended the targeted service. This suggests that both approaches are equally effective.
Parental feedback for the transition period at session 6 (antenatal) and 9 (end) of the programme.
A total of 70 surveys were completed by attendees of the universal programme. Responses to the survey were very positive. All respondents rated the course as helpful, and 93 per cent rated it as very helpful. Respondents found it a "fantastic course" and were sad to see it come to an end. They would also recommend the course to other new parents, although it was not just first-time parents who found the course useful, it could also act as a refresher for parents who already had children:
"It's been great to remind myself and my husband all the stages of pregnancy and birth, as there's been a long gap. Really nice people (tutors and other families). Turns out I have forgotten loads of things, plus loads of things have changed within these 9 years. Thank you for that!" (Parent – cloud comment) The majority of respondents (87%) rated the whole group discussions as the most helpful aspect of the course and enjoyed hearing from others in the same situation as themselves:
Being part of a small friendly and welcoming community for the last few weeks of pregnancy and post birth has been invaluable to us. We really value the level of trust and support given by working in a small group like this for an extended period of time. We have been able to ask questions we wouldn't have been able to ask elsewhere and also benefit from hearing other queries answered in discussion' (Parent – cloud comments)
The face to face delivery of the course was also important:
"The human element of the Baby Steps classes will always teach you more than books or the internet can. I have a much better idea of what to expect now" (Parent – cloud comment).
Most respondents felt the course helped them to feel more prepared to look after their baby (78 per cent strongly agree) and to feel positive about being a parent (74 per cent strongly agree):
"When I started the Baby Steps programme I did not quite realise how much support, knowledge and confidence I would gain. I am an anxious person that tends to feel low at times, during this course I have felt better than ever. This is due to the outstanding support given by all the ladies at Baby Steps! Everyone is considered and cared about in the class, the friendly atmosphere makes me and my partner feel comfortable, each week we arrive excited and ready to learn. I cannot thank the Baby Steps team enough for the guidance given over the last 6 weeks!" (Parent – cloud comment).
Ratings were slightly lower for making good friends with people in the group (49 per cent strongly agree and 35 per cent agree) and the group helping parents to improve their relationship with their partner (43 per cent strongly agree and 40 per cent agree), although this part of the programme still gained high ratings and was useful for parents:
"Made us closer as a couple, showed my partner some of the difficulties of being pregnant" (Parent – cloud comment).
Respondents were positive about the way the course had been delivered and the support of the group leaders:
"We are so grateful for everything you guys have taught us. It takes the concerns away. I particularly like all the information you gave us, but no opinions. You allowed us to make our own decisions." (Parent – cloud comment).
They also appreciated food being available for those who were attending straight from work.
It was suggested that the group could be continued after the programme. This was facilitated in one instance by a WhatsApp group. Another suggestion was to schedule a follow up group every six months or yearly to check in.
The Reach
Currently staffed for a 305 mothers/couples per annum. High number of partners are attending which is significant.
Each group is a maximum of 10 mother/partners and there are 2/3 new groups commenced each month.
The staff delivering the programme for each group remains consistent so that relationship develops over a five month period.
The staff resource currently meets demand but the universal programme is still embedding into midwifery and health visitor practice and within the local population, therefore demand could increase which there is not currently capacity to deliver within existing funding.
It is unclear to what degree parental choice plays a part in where they choose to access classes as the programme is made as a robust offer in amongst a menu of other choices that are private business predominantly.
We do continue to capture vulnerable clients within the groups but have a particular challenge where clients are non –English speaking. For this purpose then the programme content would need to be rewritten, including all resources associated with delivery and an interpreter employed and trained to deliver.
FNHC Data 2019.
Number of clients initially engaging on Baby Steps Jan- end of April 2019 (this is lightly more than a Q1 result and therefore there is some overlap with Q2)
74 women
71 partners
50 % of whom met vulnerability criteria (set out in appendix one).
Q2 data:
• 131 referrals
• 52 mums 44 partners
• 96 engaging giving an average % of 75% take up which is significantly higher than the National average in other Baby Steps
• 21 mums attended all 6 sessions (40%), 14 (31%) partners attended all 6 sessions.
(Evaluations show that attendance at 6 or more sessions increases the likelihood of gaining the outcomes of the programme).
Some reasons for not engaging with the programme initially or ongoing are shown below
Reasons why parents disengage
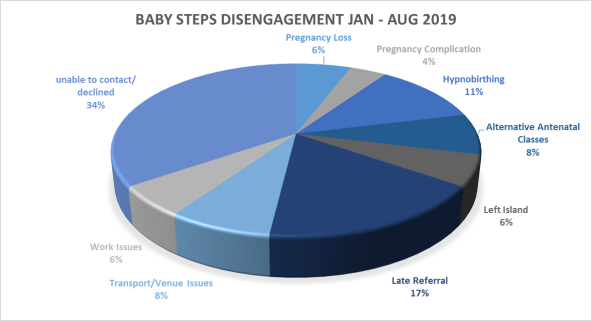
Client feedback from January 2019- Sept 2019 Survey monkey feedback 
Examples include:
Length of course was about right 93.6% First home visit was helpful -80% Topics were useful 100%
Conclusion.
The value of this programme is becoming increasingly evident as are the challenges faced and the boundaries within it is current delivery. Some fundamental issues, beyond funding, could see it improve and expand and are being progressed with the multiagency steering group. The potential is just being realised and feedback from clients and the staff supporting them is reassuring FNHC that this is the case. There is a drive and passion alongside robust evidence for the benefit of such an approach with parents which also aligns with the outcomes identified within the Children's Plan.
Appendix One
Set out below are the criteria set by the NSPCC as those clients eligible for its targeted programme delivery.
These clients continue to receive the universal offer and attend groups.
Baby Steps is for new parents who are more likely to need extra help, and less likely to access antenatal education. This includes those who:
• have drug or alcohol problems (misuse substances)
• are a recent migrant, asylum seeker or refugee
• have difficulty reading, speaking or understanding English
• have identified learning difficulties
• have low level mental health problems (might be depression or anxiety)
• are a victim of domestic abuse
• are an offender or ex-offender (committed a crime)
• are homeless
• are a care leaver
• are from a traveler community
• have no social support networks
• are in severe financial hardships (having severe money troubles)
• And/or are under 20 years of age.